
We have more than 20 years of experience in the diagnosis and treatment of infertility. We offer our patients various treatment methods, including IVF.
Fulfillyour dream of having a child with Gyncentrum clinic !


We have more than 20 years of experience in the diagnosis and treatment of infertility. We offer our patients various treatment methods, including IVF.
Fulfillyour dream of having a child with Gyncentrum clinic !
Make your first appointment at the Gyncentrum Wrocław Clinic
What is in vitro?
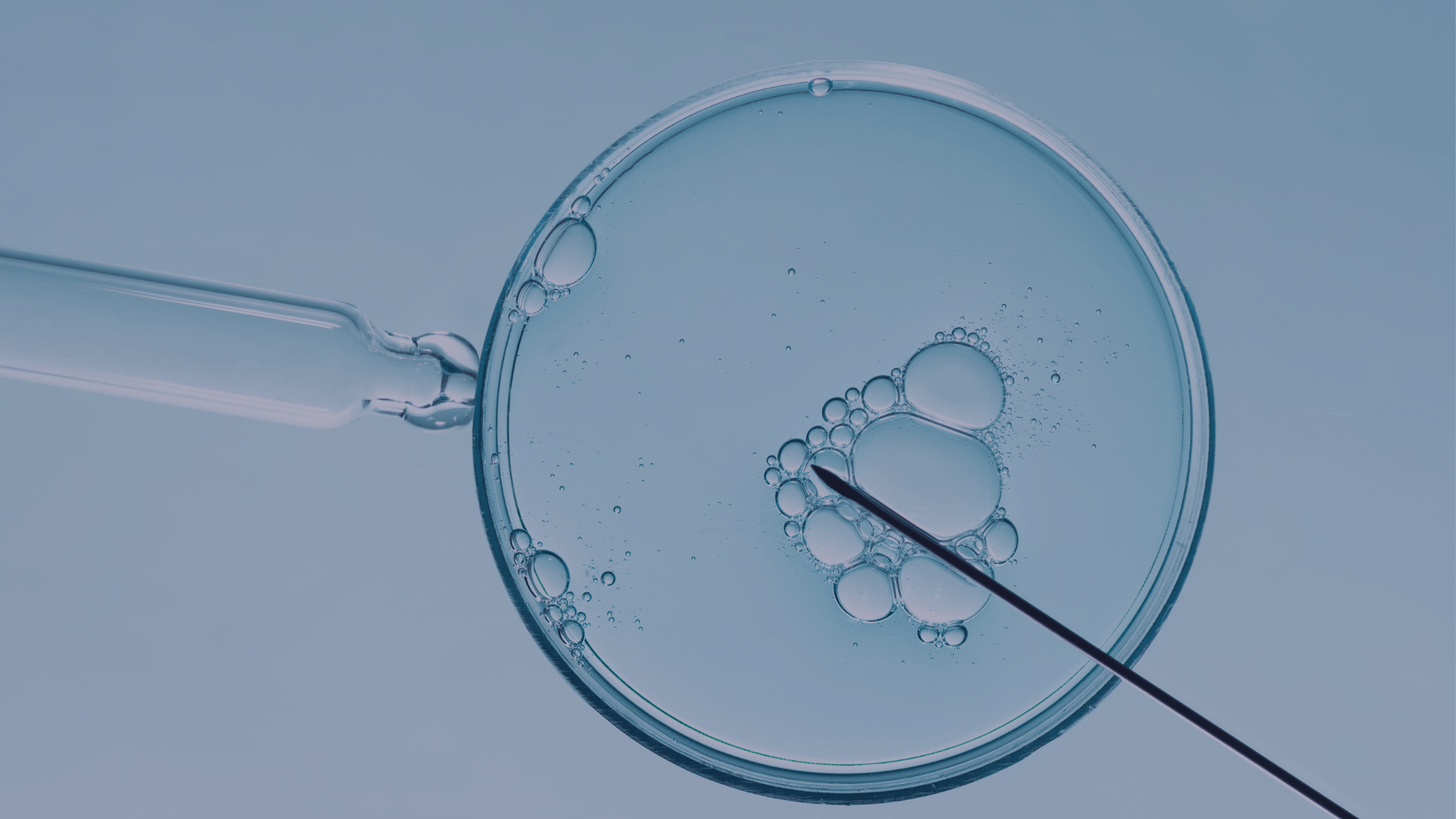
In vitro, in vitro fertilization (IVF – in vitro fertilization) is one of the methods of assisted reproduction, in which the fusion of the egg and sperm occurs in the laboratory (outside the mother’s body). The resulting embryos are placed in the uterus, where their further development already takes place.
More information >>Classical IVF, in which sperm is added to a culture dish with oocytes, is not the only method of in vitro fertilization. In addition to it, we also distinguish between :

When is IVF used?
In vitro may be indicated for both infertility occurring on the female side and on the male side.
Male
The main indications for IVF lying on the side of the man are:
Woman
For women, indications for IVF will include:

Step one: hormonal stimulation
Ovulation stimulation is a procedure in which, through hormonal stimulation of the ovaries, we are able to get more ovarian follicles than in a natural cycle. For this purpose, the patient takes hormones in the form of subcutaneous injections – according to the stimulation protocol, which is established individually by the doctor beforehand. During stimulation, the development of ovarian follicles is monitored so as to capture the best moment for ovarian puncture. It takes place when the follicles reach the required size.

Step two: ovarian puncture and sperm donation
Ovarian puncture is a procedure that completes the process of hormonal stimulation. It involves puncturing the ovaries with a puncture needle in order to retrieve the egg cells that were increased in number during the previous stimulation. The puncture procedure must be carried out within 36 hours of the patient’s intake of hCG hormone to avoid natural rupture of the Graaf follicle. The gynecologist performs a puncture of the Graaf’s follicle under ultrasound (US) guidance. He then collects the follicular fluid along with the egg cells it contains.
In the meantime, the patient’s partner – through masturbation – donates a semen sample. For this purpose, the clinic provides the man with a special room for comfort and discretion.

Step three: fusion of egg and sperm
In vitro fertilization involves the fusion of an egg cell with a sperm. This stage of in vitro fertilization takes place in the laboratory and is performed by an experienced embryologist. Before it happens, however, the egg cells are isolated from the follicular fluid and placed in special media. Semen, on the other hand, is purified and from it the embryologist selects the best quality sperm.

Step four: embryo transfer
The transfer of the embryo into the uterus, or transfer, is the culmination of the entire IVF procedure. The embryo is introduced into the uterus under ultrasound guidance using a special catheter. The procedure is performed in a gynecologist’s chair, takes only a few minutes and is judged by most women to be virtually painless. If the embryo administered to the uterus nests properly in the uterus, the beta hCG test result should be positive as early as day 10 after the transfer.
In vitro is the creation of an embryo under unnatural conditions, in glass, but with the provision of all the mimicry, that is, the resemblance of all the states that occur in natural conditions. The most common method of fusing a sperm with an egg cell is called ICSI, or under high magnification – IMSI. In the laboratory, this is done in vessels, in suitable substances that mimic the natural conditions that the oocyte would encounter in the patient’s reproductive tract in the fallopian tube and later in the uterus. The sperm is also provided with such a substrate, in which it feels like it is in the natural pathways.
First, the doctor will conduct a medical history, gynecological examination and ultrasound. He will also review the history of previous treatment. It is always a good idea to bring the results of all previous tests with you to the first visit. Based on the information gathered, the doctor will assess the patients health, present treatment options, and order additional diagnostic tests if necessary. This is also the time for the patients themselves to ask questions, so it is a good idea to prepare for the first visit in advance, for example, by writing down all the burning questions on a piece of paper. During the appointment, the doctor will ask questions such as the date of the last menstrual period, the regularity and length of cycles, the course of treatment to date. In addition, he or she may ask whether there has been a problem of infertility among family members (parents, siblings, grandparents), and about childhood and current diseases. The visit is also likely to include questions about contraceptive methods used so far, lifestyle, libido and the puberty process.
There is no one-size-fits-all set of tests that should be done before the first visit to an infertility clinic. In order for patients to get the most out of the visit and for the doctor to gather as much information as possible about the patients’ health status already at this stage, it is recommended that the woman perform basic laboratory tests, i.e. blood count, hormonal tests TSH, AMH and prolactin. The man, on the other hand, should provide the results of a basic semen test on sperm motility and physical and chemical parameters. In addition, it is worth examining sperm morphology and viability, as well as the presence of antisperm antibodies and active leukocytes.
In the case of a woman, indications for IVF may include hormonal disorders, obstruction of the fallopian tubes, low ovarian reserve, endometriosis, idiopathic infertility (of unknown cause). In the case of men, the indication for IVF is primarily low semen parameters – their insufficient number, too weak motility, errors in structure.
Yes! Today, infertility clinics have at their disposal many tools and techniques , which increase the effectiveness of in vitro fertilization. These are primarily:
The egg cell, which is given to the embryology laboratory by the attending physician during the LP, needs to be cleared of the so-called cumulus cloud, i.e. a mass of granulosa cells. Such a cell, in order to fuse it with a sperm, must be mature. When it has a clearly visible directional corpuscle, a shapely transparent sheath, if the space around the plasma is well formed and we do not have any granules, vacuoles there, then such a cell is ready for fertilization.
Semen, once donated in a special dedicated room, must be processed. We can treat it. We can remove various structures from it that would interfere with our ability to make a successful insemination. We can also sort the sperm. We do this by using a magnet – a special device that works like such a technical “maze”. After sperm is sprinkled, the sperm flows by itself into such a dedicated well, from which the embryologist then collects it. If the sperm turns out to be the right one, before we perform fertilization.
In evaluating semen, we are concerned with determining whether the sperm has a well-formed head, whether it has a well-formed acrosome, whether its movement is progressive. If there is something wrong with the sperm, we look for the causes of this condition. We are committed to selecting that best sperm, capable of fertilization.
In the embryology laboratory, we receive our partner’s sperm from our andrology department, while from the doctor we receive oocytes that are ready to be purified, and if they are mature and of the right quality, we can fuse them together with male gametes under sterile conditions, the right environment, in vitro. We expect that within several hours, two specific structures called male and female pre-nuclei will be produced and a zygote will form. Once it reaches the blastocyst stage, it is ready for implantation. We can administer it into the patient’s uterine cavity and within literally several hours expect the pregnancy to develop successfully.
After the transfer, avoid excessive physical activity and sexual contact that causes cramping. Hot baths should also be avoided.
At the time of transfer, it is recommended to administer only one embryo into the uterus. In justified cases, it is possible to transfer two – for example, when a woman is already over 35 years old and therefore less likely to implant an embryo, or is after unsuccessful attempts at in vitro fertilization. When recommending the transfer of a single embryo, the clinic is guided primarily by the patient’s well-being and wants to provide the future child with the best possible conditions for development. Transfer of a larger number of embryos is associated with the likelihood of multiple pregnancies – twins, triplets, quadruplets. Meanwhile, each such pregnancy is a greater risk of complications. Of course, all remaining embryos created as a result of the IVF procedure undergo vitrification (freezing) and are used in subsequent pregnancies.
Thawing of embryos occurs on average 2 hours before the scheduled transfer.
If there are no contraindications from the doctor the next transfer can already take place in the next cycle.
Yes, it is as possible. The whole procedure begins with the adoption of oocytes / sperm. The patient (recipient) receives oocytes taken from an anonymous donor. The donor oocytes are fertilized under laboratory conditions (in vitro) with the sperm of the recipient’s partner or, similarly, with the sperm of an anonymous donor. The resulting embryo is then transferred into the recipient woman’s uterine cavity. Indications for IVF with a donor egg are low ovarian reserve, condition after removal of both ovaries, chemotherapy, premature cessation of ovarian function.
To become a cell donor you need to meet several conditions:
The oocyte retrieval (puncture) procedure is performed under general anesthesia. Immediately after the procedure, the patient stays at the Gyncentrum Clinic in the day room for about 2 hours. After the procedure, light spotting and lower abdominal pain, similar to menstrual pain, are possible. You cannot eat, drink or chew gum for at least 6 hours before the procedure.
First of all, you must meet the following criteria:
Insemination involves the direct introduction of specially prepared semen into the uterine cavity. This is done with the help of a thin catheter, which makes it possible to bypass the barrier of cervical mucus and the antibodies, bacteria and fungi in it. The procedure is designed to increase the likelihood of the egg meeting the sperm, and thus increase the likelihood of conceiving a child. Insemination can be performed both during a natural cycle and after prior ovulation stimulation. Semen from the husband, partner or donor can be used for insemination.
It is calculated in the same way as for a pregnancy conceived naturally. Its onset is considered the first menstrual day of the cycle in which the embryo was transferred to the uterus or in which insemination was performed. If, as a result of hormonal stimulation, the menstrual cycle has shifted, the day of ovarian puncture is treated as the day of ovulation. Then 14 days are subtracted from this day (because, on average, ovulation occurs after that many days after the onset of menstruation) and it is this date that is considered the beginning of pregnancy.
Performing appropriate genetic testing before IVF allows you to better prepare for the entire in vitro fertilization procedure. It also allows to start possible treatment, increasing the chance of IVF success, i.e. conceiving and giving birth to a healthy child.
Couples undergoing IVF are advised to have a karyotype test, i.e. a set of all chromosomes.
In addition, a man should be tested for mutations in the CFTR gene, a mutation responsible for the development of cystic fibrosis, which can lead to changes in the reproductive system, such as missing or obstructed vas deferens. A third important test for a man is genetic testing of the AZF region for a microdeletion that may occur there. This is because this region contains genes encoding proteins involved in the process of sperm formation – spermatogenesis.
Women, on the other hand, are recommended to undergo genetic testing for mutations responsible for congenital thrombophilia, i.e. mutations in the gene for factor V of the blood clotting system (factor V Leiden) and the prothrombin gene. Both mutations are a major cause of the development of thromboembolism, and are also responsible for spontaneous miscarriages and other obstetric abnormalities.
Preimplantation genetic testing involves evaluating an embryo for genetic abnormalities. They are performed on cells taken from embryos created during the IVF procedure, before the woman becomes pregnant.
Early detection of defects and transfer of healthy embryos reduces the risk of reproductive failure and birth of a child with a genetic defect. Preimplantation genetic tests can diagnose Turner syndrome, Down syndrome, Edwards syndrome, Patau syndrome, Klinefelter syndrome, hemophilia, tuberous sclerosis, Huntington’s disease, cystic fibrosis, spinal muscular atrophy (SMA), Duchenne muscular dystrophy and Becker muscular dystrophy, among others.
There are several types of preimplantation genetic tests, including: PGT-A, PGT-M, PGT-SR and the newest technique for embryo genetic diagnosis – karyomapping.
Make your first appointment at the Gyncentrum Wrocław Clinic
We will contact you shortly to schedule an appointment.


